Ilomedin 20 should be used only under strict monitoring in hospitals or outpatient clinics with adequate facilities.
Pregnancy must be excluded before the start of treatment in women.
Ilomedin 20 is administered after dilution as an intravenous infusion over 6 hours daily via a peripheral vein or a central venous catheter. The dose is adjusted according to individual tolerability within the range of 0.5 to 2.0 ng iloprost/kg body weight/min.
The infusion solution should be made up freshly each day to ensure sterility.
During the first 2 to 3 days, the individually tolerated dose is established. For this purpose, treatment should be started at an infusion rate to deliver 0.5 ng/kg/min. for 30 minutes. The dose should then be increased at intervals of about 30 minutes in steps of 0.5 ng/kg/min. up to 2.0 ng/kg/min. The exact infusion rate should be calculated on basis of the body weight to effect an infusion within the range of 0.5 to 2.0 ng/kg/min. (see Tables 1 and 2 as follows for use of infusion pump or for use with syringe driver).
Depending on the occurrence of side effects such as headache and nausea or an undesired decrease in blood pressure, the infusion rate should be reduced until the tolerable dose is found. If the side effects are severe, the infusion should be interrupted. For the rest of the treatment period, therapy should be continued with the dose found to be tolerated in the first 2 to 3 days.
The blood pressure and heart rate must be measured at the start of the infusion and after every increase in the dose.
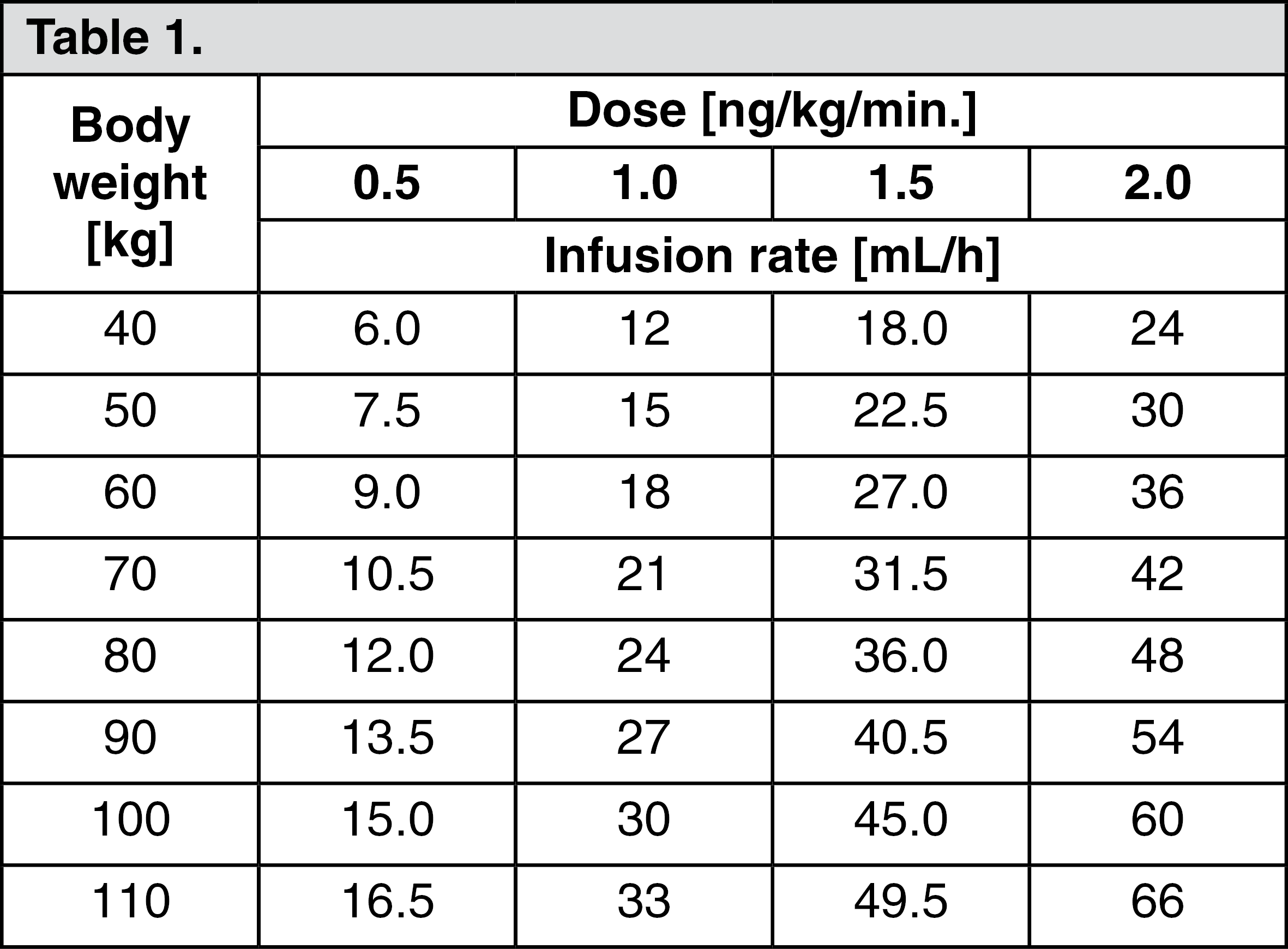
Infusion rates [ml/hour] for different doses for use of infusion pump: In general, the ready-for-use infusion solution is infused intravenously by means of an infusion pump (e.g. Infusomat). For this purpose, the contents of a 2.5-ml ampul (i.e. 50 μg) of Ilomedin 20 are diluted with sterile physiological saline solution or a 5% glucose solution to the final volume for infusion of 250 ml, and the contents of a 1-mL ampul (i.e. 20 μg) of Ilomedin 20 are diluted with sterile physiological saline solution or a 5% glucose solution to the final volume for infusion of 100 ml. The contents of the ampul and the diluent should be mixed thoroughly. In the case of an Ilomedin 20 concentration of 0.2 μg/ml, the required infusion rate should be determined according to the previously described scheme to effect a dose within the range of 0.5 to 2.0 ng/kg/min.
(Please interpolate to match the patient's actual body weight, then set the infusion rate to the target dose in ng/kg/min.) (See Table 1.)
 Click on icon to see table/diagram/image
Infusion rates [ml/hour] for different doses for use of syringe driver:
Click on icon to see table/diagram/image
Infusion rates [ml/hour] for different doses for use of syringe driver: A syringe driver with a 50-ml injection syringe (e.g. the Perfusor) may also be used. In this case, the contents of one 2.5-ml ampul (i.e. 50 μg) of Ilomedin 20 are diluted with sterile physiological saline solution or 5% glucose solution, to reach a final volume of 25 ml, and the contents of one 1-ml ampul (i.e. 20 μg) of Ilomedin 20 are diluted with sterile physiological saline solution or 5% glucose solution to reach a final volume of 10 ml. In the case of an Ilomedin 20 concentration of 2 μg/ml, the required infusion rate should be determined according to the previously described scheme to effect a dose within the range of 0.5 to 2.0 ng/kg/min.
(Please interpolate to match the patient's actual body weight, then set the infusion rate to the target dose in ng/kg/min.) (See Table 2.)
Click on icon to see table/diagram/image
The duration of treatment is up to 4 weeks. Shorter treatment periods (3 to 5 days) are often sufficient in Raynaud's phenomenon to achieve improvement over several weeks.
It should be borne in mind that iloprost elimination is reduced in patients with renal failure requiring dialysis and in patients with liver cirrhosis. In these patients a dose reduction (e.g. half the recommended dose) is necessary.
Continuous infusion over several days is not recommended because of the possible development of tachyphylaxis of platelet effects and the possibility of rebound platelet hyperaggregability at the end of treatment, although no clinical complications associated with these phenomena have been reported.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image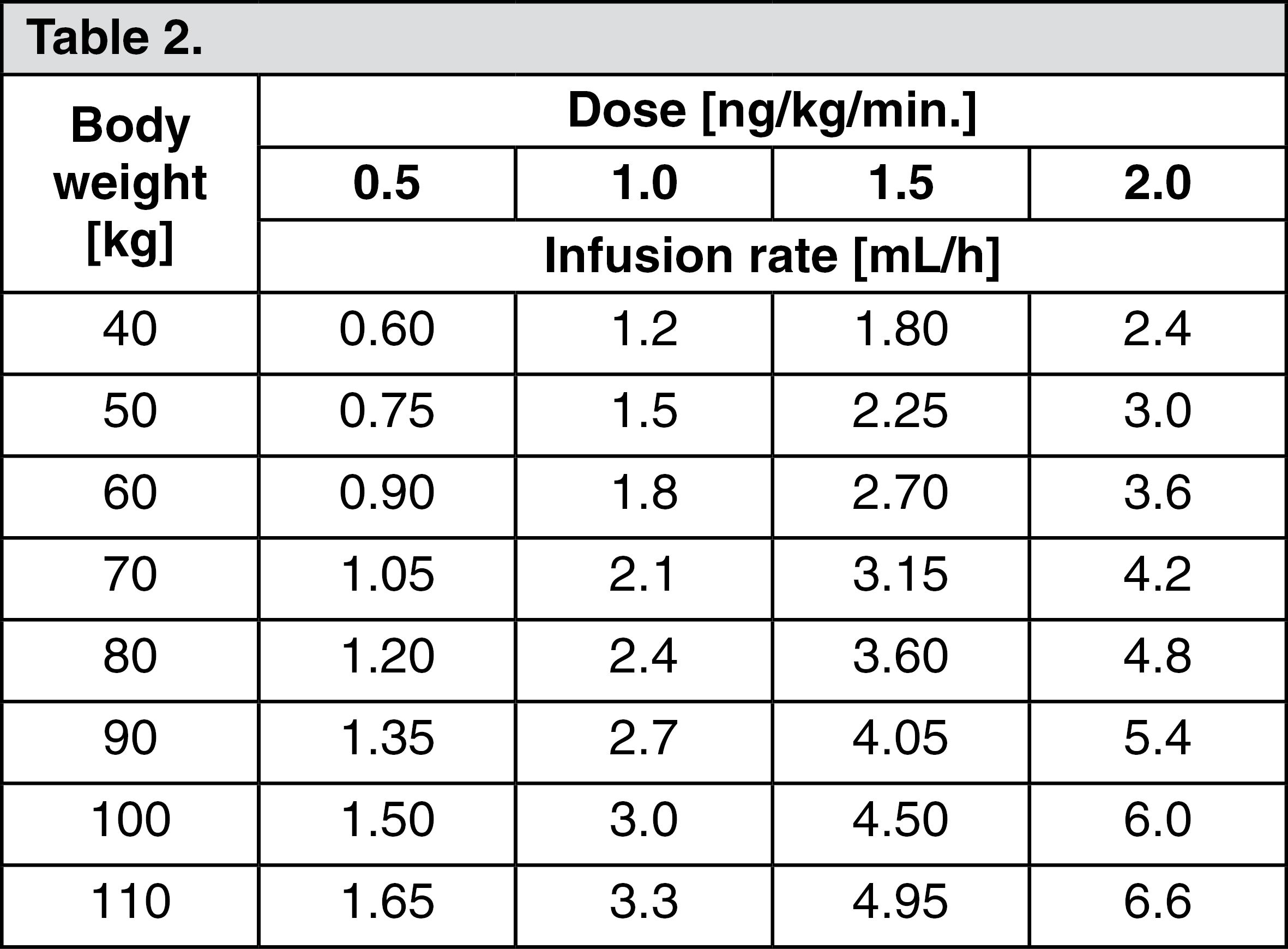 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image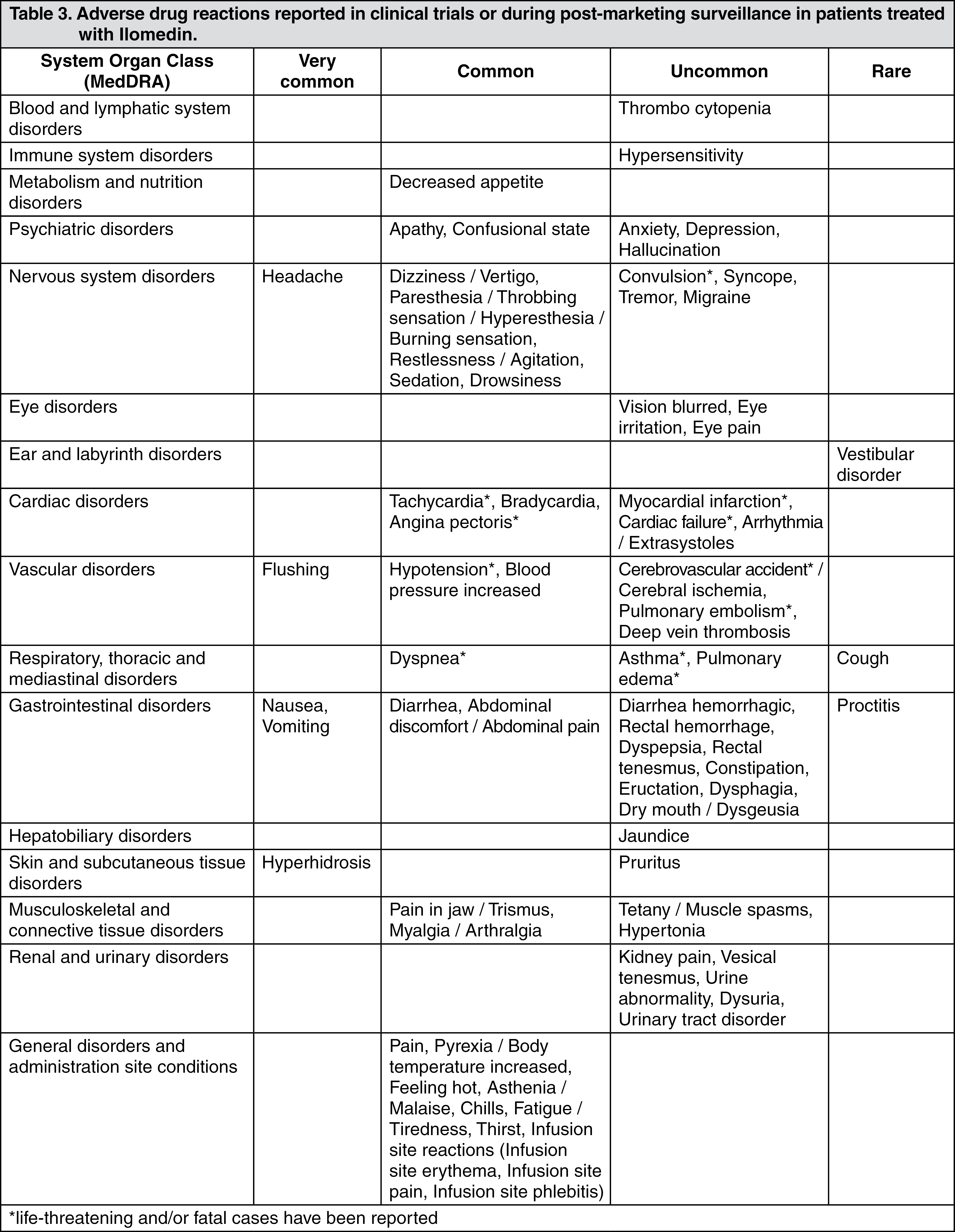 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out